Patients suffering from depression,epilepsy and psychosis will soon have access to treatment at the primary healthcare, PHC, level in Lagos, if a new project initiated by Mental Health in Primary
Care (MeHPriC),through grants from Grand Challenges Canada (GCC) is anything to go by.
The new project which is the first of its kind in Nigeria is aimed at closing the gap in mental health management created by shortage of psychiatrists in the country.
It is also to shift the task of treatment to doctors and other health workers at PHC level to ensure only more chronic conditions are referred to tertiary facilities.
In chat in Lagos, Principal Investigator, Mental Health in Primary Care, MeHPriC, Dr. Abiodun Adewuya, explained that the programme is being funded by the Grand Challenges Canada, GCC, while the Lagos State University College of Medicine, LASUCOM, will manage the grant. The Lagos State Ministry of Health and Lagos State Primary Health Care Board,LSPHCB, are involved while the Centre for Mental Health Research and Initiative, CEMHRI, and the Institute of Psychiatrics, London are the other partners.
Adewuya said a research was conducted to implement and evaluate intervention for depression, epilepsy and psychosis tagged DEP in primary care in five divisions in Lagos called IBILE.
“The programme will ensure that each division under IBILE, which is an acronym for Ikeja, Badagry, Ikorodu, Lagos Island and Epe, covers five million persons living with Depression, Epilepsy and Psychosis, DEP.
Lamenting that Nigeria has less than 300 psychiatrists he said, just 32 currently worked in Lagos State.
Adewuya, who is also the Head of Department of Psychiatry, Lagos State University Teaching Hospital, LASUTH, said doctors, nurses and other health care workers at the PHC, will be trained to identify and treat DEP so that there would be increased access to evidenced-based intervention and improved health outcome in clients with DEP receiving the treatment.
Co-investigator, Prof Martins Prince said DEP under the project can be treated by building the capacity of doctors, nurses and other workers at the PHC level to identify their signs and symptoms.
Prince, a professor of psychiatry at the Institute of Psychiatry, Kings College, London, identified major problems of mental health as under-diagnosis and under-treatment.
“We call the problem treatment gap. This is why the World Health Organisation programme is called MHgap. It is a global action plan. Mental health gap is about closing that treatment gap. The treatment gap is big actually in high income country such as the United Kingdom, probably about half of the people with depression in the UK go without treatment. But the treatment gap in low and middle income countries such as Nigeria are absolutely huge.
“In rural area of Africa, 90 per cent of people with psychosis never had treatment or care. Two-thirds of people living with epilepsy which is associated with stigma never had any treatment to their condition. We think four out of five people, which is 80 per cent in Nigeria, have serious episode of depression and do not have treatment. There is little awareness and people don’t seek help and even if they do, it is through the traditional healers not from the bio-medical system,” Prince said.
He noted that one of the biggest barriers was dearth of specialists. “There is lack of adequate psychiatrists, psychologists, community mental health nurses, which is why there was no specialist to take on this disease burden directly. So what we need to do is to mobilise the forces of public health in particular primary health care to be providing much of the treatment to the priority mental and neurological disorders which currently they don’t do, they are not trained for it and no expectation that they should do it nor see it as part of their job.
But there is no reason why they shouldn’t be engaged in this way. This will reduce the barriers and cut the cost of treatment and make treatment more accessible and reduce stigma.
“Fundamentally what we are doing is that we are engaging in task sharing, we are using the specialist to advise, train and to supervise the non-specialist who are much greater in number to actually learn to be providing much of the combine treatment.
Depression affects one in seven in a PHC while psychosis affects about one per cent of the population. They are very chronic, disabling and serious condition where treatment can make a big difference to the outcome.
“If people with depression receives anti-depressant and people with psychosis receives anti-psychotic medication and support reabilitation at the community the outcome will greatly improve.”
Adewuya said 13 people, which include three doctors, five nurses, three community health extension workers (CHEWS), one pharmacy technician and one social worker will be trained per each flagship PHC centre in each division. “Approximately 200 people are expected to receive the training,” he said.
ABUJA: Training Schedule for Basic Life Support BLS, Pediatric Advanced Life Support (PALS), Advanced Cardiovascular Life Support ACLS, First Aid, CPR, AED
PORTHARCOURT: Training Schedule for Basic Life Support BLS, Pediatric Advanced Life Support (PALS), Advanced Cardiovascular Life Support ACLS, First Aid, CPR, AED
LAGOS: Training Schedule for Basic Life Support BLS, Pediatric Advanced Life Support (PALS), Advanced Cardiovascular Life Support ACLS, First Aid, CPR, AED
STOP paying for airtime and electricity, Let your phone pay its bills with ScreenT
You may also like

PSN Raises Alarm as 3 Million Illegal Drug Outlets Threaten Public Safety
The Pharmaceutical Society of Nigeria, PSN, in Lagos State yesterday warned…

Agencies move to strengthen early warning systems in Nigeria’s healthcare sector
Key government and international agencies have intensified efforts to stren…
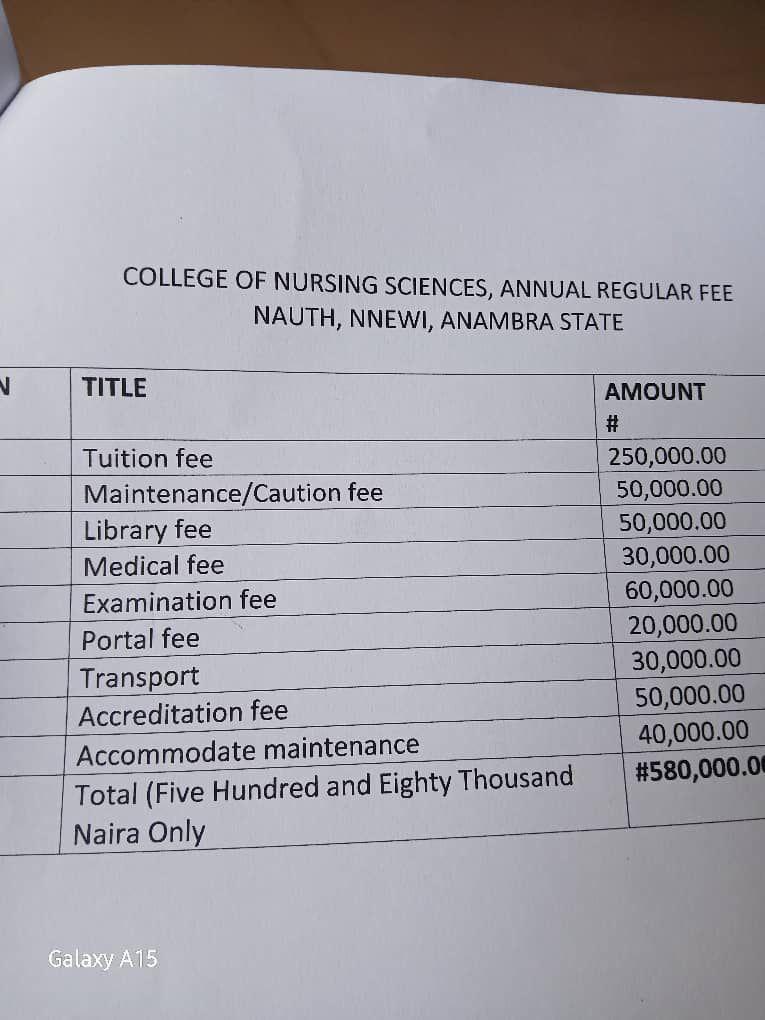
NAUTH management moves to resolve tuition hike protest, promises dialogue with students
The management of Nnamdi Azikiwe University Teaching Hospital (NAUTH) has p…

Child health outcomes improve as facility-based maternal deaths decline in 2025 FG report
The Federal Government has reported significant improvements in maternal, n…

World Kidney Day: Caregivers groan as dialysis hits N80,000 per session, transplant N30m
As the world marks World Kidney Day, caregivers and health experts in Niger…
