In the western world, people usually don’t make a distinction between illness and disease. These two terms seem to mean essentially the same thing and are often used interchangeably. However, it is important to define illness and disease differently when considering some non-western cultural traditions.
Disease is an objectively measurable abnormal functioning of the body system like tooth decay, measles or a broken bone. This is the term that deals with the bulk of consultations that get the attention of our surgeons and physicians. Illness, on the other hand, is a feeling of not being normal or healthy, which may not be objectively appraised, as it could be linked to psychological or spiritual imbalance.
The majority of disorders treated by the psychiatrists fall into the category of illnesses, which invariably determines the concept of attainment of cure. This determination of cure or otherwise is largely determined by the proposed understanding of its cause from the world view of the patient.
Trained medical personnel can determine and demonstrate empirically the cure of diseases through a gamut of clinical examinations and laboratory investigations. As diseases get treated, there may be empirical correlations between the patient’s subjective experiences and empirical demonstration of recovery in both the clinical examinations and the laboratory investigations. However, for mental illness, there is no clear-cut demonstrable cause that could be taken to the laboratory to be investigated, apart from clinical interviews in the therapeutic relationship. The determination of cure or the measurement of recovery becomes very difficult and challenging in the case of mental illness.
The factors held to be the cause of mental illness are often diverse and multiple, ranging from the psychological to the cultural and even to the spiritual, hence the difficulty in objectively determining the recovery from mental illness.
However, what is certain is the experience of the patient, especially in terms of the remission of the symptoms and the cessation of the distress caused by the symptoms. Although the side effects of the interventions applied may pose some minimal challenges, this does not detract from the observable and demonstrable relief of distressful experiences of the patient.
.jpg)
Morbid thought patterns, such as accusing relatives or spouses of planning to harm the victim, actually disappear when medications are administered; just as hearing voices of unseen personalities stop.
The gravity of distress caused by these morbid thoughts, or hearing voices that disturb thoughts and concentration, is unimaginable.
This relief of distress that invariably helps patients to resume occupational and social functioning facilitates the concept of cure in medical practice, since no illness or disease is absolutely cured without the possibility of recurrence.
The World Health Organisation recognises this concept of cure and therefore redefines health as not only the absence of disease or infirmity, but a state of complete physical, emotional and psychological well-being.
This definition takes the perception of cure from the narrow paradigm of clinical appraisal into a more global psychosocial definition. It is possible for someone to recover from a disease, but he may not be psychologically sound as a result of other issues in the background of his life, even though the laboratory parameters are unequivocally normal.
The importance of a subjective viewpoint of recovery from illness led to the development of a method that is patient-centred. Whether it is a disease or an illness, the perception of the patient being treated is the most crucial assessment, irrespective of the laboratory or clinical parameters. It follows, therefore, that the measurement of health and the effects of health care must include not only an indication of changes in the frequency and severity of diseases, but also an estimation of well-being. This can be assessed by measuring the improvement in the quality of life related to health care.
Although there are, generally, satisfactory ways of measuring the frequency and severity of diseases, this is not the case in so far as the measurement of well being and quality of life are concerned.
The WHO developed an instrument through collaborative work of about 15 field centres around the world, through which important aspects of quality of life and ways of asking about quality of life were drafted on the basis of statements made by patients with a range of diseases, by people who are not ill, and by health professionals in a variety of cultures.
The WHO defines the quality of life therefore as an individual’s perception of his/her position in life in the context of the culture and the value systems in which they live and in relation to their goals, expectations, standards and concerns. The patient therefore is the focal issue in the pathway of recovery.
By ADEOYE OYEWOLE
The Punch
ABUJA: Training Schedule for Basic Life Support BLS, Pediatric Advanced Life Support (PALS), Advanced Cardiovascular Life Support ACLS, First Aid, CPR, AED
PORTHARCOURT: Training Schedule for Basic Life Support BLS, Pediatric Advanced Life Support (PALS), Advanced Cardiovascular Life Support ACLS, First Aid, CPR, AED
LAGOS: Training Schedule for Basic Life Support BLS, Pediatric Advanced Life Support (PALS), Advanced Cardiovascular Life Support ACLS, First Aid, CPR, AED
STOP paying for airtime and electricity, Let your phone pay its bills with ScreenT
You may also like

PSN Raises Alarm as 3 Million Illegal Drug Outlets Threaten Public Safety
The Pharmaceutical Society of Nigeria, PSN, in Lagos State yesterday warned…

Agencies move to strengthen early warning systems in Nigeria’s healthcare sector
Key government and international agencies have intensified efforts to stren…
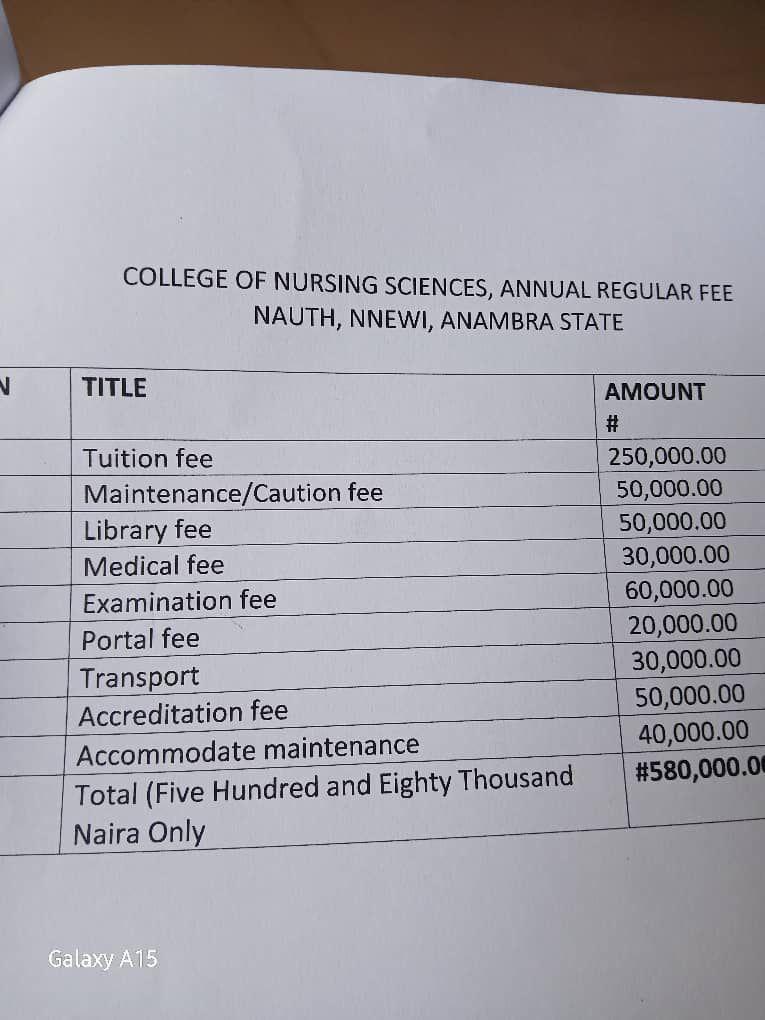
NAUTH management moves to resolve tuition hike protest, promises dialogue with students
The management of Nnamdi Azikiwe University Teaching Hospital (NAUTH) has p…

Child health outcomes improve as facility-based maternal deaths decline in 2025 FG report
The Federal Government has reported significant improvements in maternal, n…

World Kidney Day: Caregivers groan as dialysis hits N80,000 per session, transplant N30m
As the world marks World Kidney Day, caregivers and health experts in Niger…
