Women giving birth with no one present are mostly subsumed under deliveries unattended
Asabe Balarabe spent years in nursing and knew all about delivering, but customs made her choose to give birth at home. Women in her culture go to their parents’ home to give birth, and then return to their marital homes after 40 days.
Even before she went to her mother’s house, Asabe knew she couldn’t deliver her baby, it was big and in breach: she knew this from the antenatal clinic she visited.
Her mother plied her with herbs and prayers.
“When the labour started, she said I should not tell anybody and that I will deliver safely,” Asabe recalls. “I tried and tried until I observed the baby was in distress. My mum still insisted that I could deliver at home.”
“Luckily for me, one of my uncles came around and said I should be taken to the hospital.”
Surgeons did a caesarean section to bring out the baby, but Asabe would stay in hospital for three weeks: an infection had already set in.
Balarabe tried to deliver with no medical personnel present. That she failed and went to hospital is seen as weak among certain customs. Up to a million women give birth with no one present, according to a new research using data from the National Demographic Health Survey.
And no one present means that-absolutely none present, skilled or unskilled.
“The category of no-one-present and some-one-present is always lumped together in the studies conducted in Nigeria, and so we haven’t been able to pay attention to this segment of women who deliver with no one present,” said Dr Bolaji Fapohunda, researcher at John Snow Inc, which implements the Targeted State High Impact Projects (TSHIP) funded by the US government in Nigeria.
Why would women choose to give birth by themselves?
“One, is the culture, two, is lack of education, three is poverty and the fourth is the health system itself,” according to Dr Habib Sadauki, Country Director for Fistula Care, a project funded by USAID to treat and support women with obstetric fistula.

“The health system is not in the best of shape to provide the required services because they lack personnel or inadequate supplies in the hospital. If you resolve the issues in the hospital with improved services you are most likely going to see a change and you can also work in the community in the needed areas. But in the long term what you need is an overall education in the whole northern Nigeria,” Sadauki explains.
“What that means is that the decline is not happening as speedily as we will like to see it in the number of women who deliver with no one present across the country. It is predominantly concentrated in the north western part of the country because around one million per year still do that,” says Dr Nosa Orobaton, co-researcher in the study published in the International Journal of Women’s Health.
“What this means is that women who live in rural areas, who have lower income and women who have lower education are likely to deliver with no one present.”
Intervention to stop births with no one present started in Sokoto in 2008, when 25% of all births fell into that category.
Interventions ranged from sensitization and dialogue with audience who had negative perceptions about childbirth, says Sani Jabbi, a traditional ruler in Sokoto State.
“We also strengthened the capacity of communities to own their health care systems and the reactivated existing health structures in the state,” Jabbi says.
A community-based intervention to distribute misoprostol (to prevent bleeding after delivery) and chlorhexidine (to prevent infection of a newborn’s cord) which placed a health volunteer with every pregnant woman who delivered at home also helped to reduce maternal and neonatal deaths.
In 2013, five years later, births with no one present accounted for less than 1% of all births, according to a study of the intervention by TSHIP.
Halima Yusuf, a social worker has learnt not to rely on experience: every child birth is quite different, she explains.
Yusuf says: “When I was to have my third baby, I was advised to have my baby at home but I declined because I had never had any baby at home. The experience
I had with my first two babies was not the same as the third. I had a long labour this time. The baby wanted to come out but there was something hindering it, so I called the nurse. When she examined me, she noticed that there was a cord around the neck of the child. She asked me to stop pushing and relax. She took an instrument and clamped the cord and in few minutes the baby came out. If it was in the house, they may not detect this and even if they do, they may not have the equipment to do that.”
Balarabe’s second labour started with a sharp pain in her abdomen and then bleeding.
Her mother told her to wait, “but I told her I would not wait for her this time. Before she could get a car to take me to the hospital, I collapsed because I was vomiting and at the same time bleeding,” Balarabe recalls.
Her baby was stillborn, she was given five-pint blood transfusion and had to stay in intensive care and on oxygen tanks.
Now a midwife at Amanawa General Hospital, Sokoto, has a message: “What I preach now is that women should go to the hospital for antenatal and to deliver their babies in hospitals where they can get professional help, not stay at home.”
by Victoria Onehi
Daily Trust
ABUJA: Training Schedule for Basic Life Support BLS, Pediatric Advanced Life Support (PALS), Advanced Cardiovascular Life Support ACLS, First Aid, CPR, AED
PORTHARCOURT: Training Schedule for Basic Life Support BLS, Pediatric Advanced Life Support (PALS), Advanced Cardiovascular Life Support ACLS, First Aid, CPR, AED
LAGOS: Training Schedule for Basic Life Support BLS, Pediatric Advanced Life Support (PALS), Advanced Cardiovascular Life Support ACLS, First Aid, CPR, AED
STOP paying for airtime and electricity, Let your phone pay its bills with ScreenT
You may also like

PSN Raises Alarm as 3 Million Illegal Drug Outlets Threaten Public Safety
The Pharmaceutical Society of Nigeria, PSN, in Lagos State yesterday warned…

Agencies move to strengthen early warning systems in Nigeria’s healthcare sector
Key government and international agencies have intensified efforts to stren…
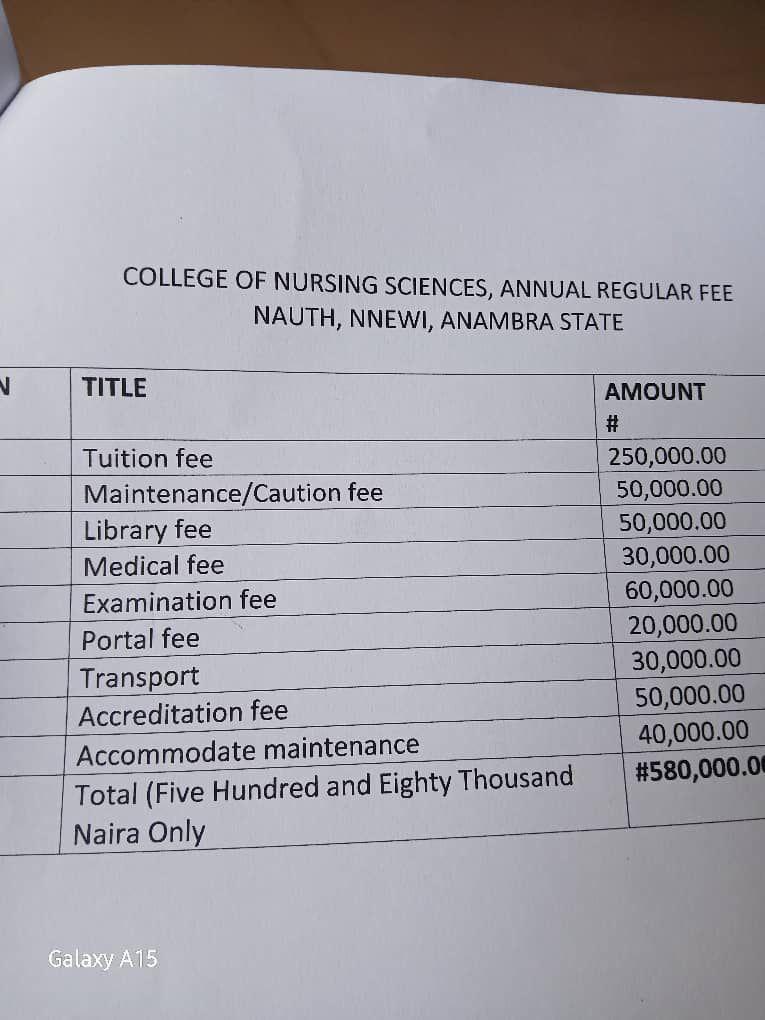
NAUTH management moves to resolve tuition hike protest, promises dialogue with students
The management of Nnamdi Azikiwe University Teaching Hospital (NAUTH) has p…

Child health outcomes improve as facility-based maternal deaths decline in 2025 FG report
The Federal Government has reported significant improvements in maternal, n…

World Kidney Day: Caregivers groan as dialysis hits N80,000 per session, transplant N30m
As the world marks World Kidney Day, caregivers and health experts in Niger…
