Dr. Mike Omotosho is the Managing Director/ Chief Oversight Officer of Sustainable Healthcare Initiative (SHI). A Certified Manager of Successful Programmes and Chartered Manager of Risks in Projects; with 20 years experience in Programmes Management, Health Commodity Logistics, sales, marketing, business development and strategic management. He trained as a pharmacist from Ahmadu Bello University Zaria and has a Masters in Business Administration from Business School Netherlands. In this interview, he speaks on the seeming unending crisis in the health sector and proffers ways to resolve it. JOKE FALAJU writes from Abuja. Excerpts:
HOW do you see Nigeria’s health sector that is currently enmeshed with crises?
It is a very depressing situation; {because just two weeks ago, I lost a friend who was then in need of an open heart surgery. You wouldn’t believe that they searched all across hospitals in Abuja; they couldn’t find… he died. He was a Liberian and a lot of us around liked him. We didn’t know he’s Liberian until he died because people called him Chinedu; and he had become part of us.
He is not the only person because} I’ve just read in the newspaper that a lady died with twins while trying to give birth. I am sure there are several stories like that if you look around. It is totally depressing. My understanding, which I strongly hold on to, is that health care is all about the patient. It is about who should be crowned king – the patient, and then who is in charge of the others. It is about the patient, and it is so sad that people are missing the point.
I see a situation where everybody would sit around the table and say ok, we have the patient as the central point, how do we all contribute to make patient care a lot better? Instead, we are fighting ourselves over who is in charge of health and care. It is totally depressing. The situation we are in right now is the same situation where our fellow countries were several years; where each health professional held on to what they believed they should be doing.
People have moved far beyond disciplinary health care. Right now, most countries are deploying what I call inter-disciplinary health care; where the various disciplines are there, they are recognized, you come to the table with your expertise and the other person comes with his expertise and I come with mine, and we all sit together and say how do we make the patient a lot better? This is because it is all about the patient, the way a salesman will tell you that costumer is the king. In health care sector, patient is king. It is not about me as a pharmacist or you as a doctor or her as a nurse; or even the lab scientist. Everybody is respected; everybody comes to the table with something. But, the focus is the patient. I wish our colleagues will understand this central point and then come to the table.
Can the present situation in which we have found ourselves help global advocacy for task-sharing in health services?
That is exactly the point we are making. Task sharing slightly differs from what we are advocating. Task-sharing is an integral component of interdisciplinary approach to patient’s care. Task-sharing simply means as a pharmacist, do I understand a bit of what the doctor can do? Or do I understand a bit of what the nurse can do? Or do I understand what the lab scientist can do? This means that if the lab scientist is not there, I may be able to carry out the test that the lab scientist could do. That is what we are saying. You will see that that itself is an advantage of the team work I am talking about. I probably will not go to school to study medical science or lab science. But, when people work together as a team, share experience, I will understand a bit of what each person working on the team is doing. Whenever there is a lacuna, it becomes a lot easier for anybody to step in.
So, for me, I will not immediately advocate task-sharing as it is. I will advocate inter-disciplinary approach to patient care. Then, automatically, task-sharing will become one of the advantages that we will enjoy. They are similar, but there is a very tiny difference because with task-sharing, yes, everybody will be able to do something a little bit of somebody else. The doctor will be able to dispense medication, which is easy. The pharmacist will be able to diagnose in simple cases, not complex ailment. And, then, perhaps, the doctor will be able to set up a line where the doctor is not available even though it is doctor that is supposed to do that. But, I am saying, yes, that is allowed, but that is not supposed to be our focus.
When you come with that approach, because looking at our health sector now, people will begin to say someone else want to take their jobs, but that is not the case. But, if you say oh, we are coming together as a team; it is not your job that is the issue. Bring what you have, he brings what he has, everybody works. It is the patients that we all focus on. Then, it becomes a lot easier to learn from each other and then task-share when the need arises as against making it the key point.
Strike has been tool for flaunting professional might in the health sector, what do you think government should do to bring peace to the sector?
First and foremost, I think that all warring parties must be brought to the table, as a pharmacist for instance, I have a whole lot of respect for medical doctors by virtue of their training, by virtue of the duration they spend and even by virtue of the relevance when it comes to patients’ care. They are the natural leaders. But, don’t forget that leadership starts by being a follower. You can’t lead when there is nobody following. And, these days, it is beginning to change. People understand that the definition of the patient’s illness determines who takes the lead in the patient care. Yes, they (doctors) are natural leaders, then, it doesn’t mean you’ve got to lead all the time. At times, the kind of ailment will determine who should take the lead.
So, let everybody come back to the table and say ok, we are all working together and you cannot lead outside the team. You cannot lead without a follower; and that is very important. I think everybody should come to the table and understand that the patient is the most important part. There is no point fighting for relevance and the patients are dying on a daily basis. You’ve sworn oath to protect their lives to the best of your ability. You now because of relevance on the table of who leads want to determine the growth pattern of other health care partners within the team while the patients die. I think there is anomaly, I can’t just understand that.
I think everybody should come to the table, we should begin to encourage team work, and we should begin to practice inter-professional approach like I said. I was giving you the graduation, you have your separate discipline like the doctors would have, pharmacists, medical lab scientists and nurses, you have your discipline, I agree. But it doesn’t work well when you begin to tell government this is what I do, no! Overtime, we come together, and then, it becomes a multi-disciplinary approach. When you are doing yours, the nurse is doing his, everybody is doing it but in the same set up.
But, if they do not communicate with each other, then, it is still multi disciplinary. The inter relationship between them is what makes it interdisciplinary. First, there has to be that coordination where you define the role for everybody. Everybody knows their roles. I don’t have to overstep my boundary. The emphasis here is not about who leads; it is about the patient who is king.
So, when we define the roles, then, we will get to communicate. After communicating with each other, it now becomes easier to have a shared responsibility with the patient. Please, get me right, I am not talking about sharing our responsibility, no. But, there must be a shared responsibility towards the patients. Pharmacist knows I’ve got to ensure the patient is ok; doctor knows too that he’s got to ensure the patient is ok. If there is no coordination, there is no effective communication, then, there is no way the can have that shared responsibility to ensure that the patient is ok, which should be a central focus. My call will be that everybody come together and let’s begin to practice well. It is not late.
Are you saying the strike embarked upon by the doctors is not justified?
Yes, it is not justified. There is no amount of logical argument that will justify the loss of life of a patient. That is what I am saying. Irrespective of what those 24 demands by the doctors are, no, and I will tell you something. Your candle will not be brighter by putting off my own candle. But, if you have me light my candle and you light your own, the room becomes brighter. We must all work together. So, there is no justification, no moral justification to lose the thousands that have died during the strike.
Can multi-disciplinary approach work in the Teaching Hospitals, which is one of the issues in contention?
That is exactly the point I am making. Like I said, the medical doctors by the virtue of all of those are the natural leaders. But, we need to understand that it is not about who leads, it is about the patients. I tell you, this can work everywhere because the doctors will come in, the nurses will come in there because the teaching hospitals are not there for doctors alone. It is for everybody. You have pharmacists that actually go to teach doctors, they teach them pharmacology. You have doctors that come to teach pharmacy too. We even have nurses that go to teach doctors as the case may be. It is about what you have that you want to impact on the other person.
The assertion that it is only the person that is teaching somebody that is relevant doesn’t work all the time. Haven’t you heard of a case of the students even becoming more relevant that the teachers? That is even if it is true that it is doctor that is teaching everybody. Let’s not join issues with irrelevance. Let’s concentrate on the point itself. Once everybody begins to understand the importance of coming together as a team, I come with my professional expertise at the table, the patient is central. You notice I have been repeating this because that is the message. The patient is the central point; I come with my own core skills as a pharmacist. You come with your core skill as a doctor. You come with your core skills as a radiologist. Everybody has a role to play. It is the patient that matters.
At the end of the day, especially in Teaching Hospital as you are saying, the cost of care becomes more effective, the care becomes more effective. The cost becomes lower. And, more importantly, you have a wide array of services provided within that small community. Who benefits the most? It is the patient because it is all about the patients.
What is your appraisal of government in making this sector work?
I think judging by where we are now, and taking a step back retroactively to where we are coming from, I will say that the government has done tremendously well. Of course, it is a far cry from where I want to see it. But, the government is not taking care of things well because you have a system where everybody works his own way. I am quick to tell people, I think there has to be a reawakening of our core professional duties as individual player in the health sector. We need to make everybody understand that the patient is still king. I have my own skills but I am going to use it to make the patients better; that is it. And, this must start from school; from the training. Like I said, there are natural leaders; like I said, I respect doctors. The same way I respect my professional colleagues, pharmacists, the same way I respect what the medical lab scientists bring to the table, the same way I respect the nurses, I respect what everybody brings to the table.
Let me give you a simple example, in the whole of this building, we have just about four toilets. Just imagine that our janitor doesn’t come to work one day. And, about 40 people go into the toilets. Do you think you will be able to able use the toilets at the end of the end when not cleaned? That day, will begin to appreciate that janitor. It is as simple as that. It is all about team work. No matter how relevant you are as a team, if only part of the team appears, the team is only as strong as the weakest link.
At what point did the issues we are facing in the health sector begin?
It has been an old age rivalry. That is the reality. I am just saying that our fellow countries have grown out of them and we are just there. We should take a clue from what is happening. By virtue of the training, the quality of interaction with the patient, the duration of the training, the bulk of work; the doctors are natural leaders. So, it is already in their psyche that yes, they lead. Like I said, leadership is about followership; leadership is about team work. So, the moment they understand that yes, I am a leader, I am in charge here. But, then, the relevance of everybody is very important. And, we now say ok, the patient that we are all struggling to satisfy is the king; not who leads, not who is in charge. Once you make the patient the fulcrum of all of the discussion, you will find out that who leads become irrelevant. The natural leader will continue to lead; no problem.
What is your final call on this strike?
I say as a country, we need to step up our game. We need to stop all the bickering, come back to the table and put the patient first. If you care about the patient, you will agree that there is no amount of logical explanation that will suffice for the loss of a single life. We should drop all the criticisms, all the blames and all the struggles for relevance and who leads.
ABUJA: Training Schedule for Basic Life Support BLS, Pediatric Advanced Life Support (PALS), Advanced Cardiovascular Life Support ACLS, First Aid, CPR, AED
PORTHARCOURT: Training Schedule for Basic Life Support BLS, Pediatric Advanced Life Support (PALS), Advanced Cardiovascular Life Support ACLS, First Aid, CPR, AED
LAGOS: Training Schedule for Basic Life Support BLS, Pediatric Advanced Life Support (PALS), Advanced Cardiovascular Life Support ACLS, First Aid, CPR, AED
STOP paying for airtime and electricity, Let your phone pay its bills with ScreenT
You may also like

Agencies move to strengthen early warning systems in Nigeria’s healthcare sector
Key government and international agencies have intensified efforts to stren…
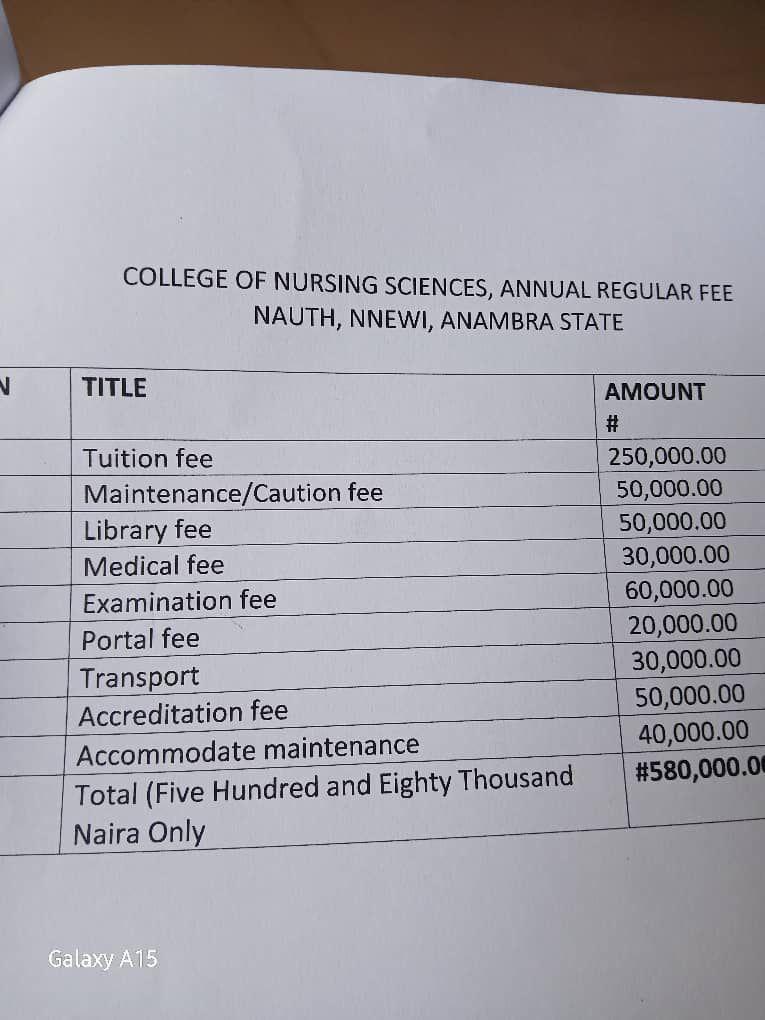
NAUTH management moves to resolve tuition hike protest, promises dialogue with students
The management of Nnamdi Azikiwe University Teaching Hospital (NAUTH) has p…

Child health outcomes improve as facility-based maternal deaths decline in 2025 FG report
The Federal Government has reported significant improvements in maternal, n…

World Kidney Day: Caregivers groan as dialysis hits N80,000 per session, transplant N30m
As the world marks World Kidney Day, caregivers and health experts in Niger…

FG receives long-acting injectable Lenacapavir for HIV prevention
The Federal Government has received supplies of the long-acting injectable …
