One of the biggest health problems today in our part of the world is malaria. Among every five live births in sub-Saharan Africa, one will die from malaria before the age of five years. It is a very sobering statistic indeed and thousands of young children die every day from the direct effects of this disease. In each year, some 2 million people die from malaria. It is common in other parts of the world such as Asia and the Americas. It is prevalent in those parts of the world that have a tropical or subtropical climate where warm temperatures, high levels of humidity and bodies of stagnant water provide the ideal environment for the mosquito larvae to breed. It is caused by the bite of an infected mosquito which harbours the parasite and thus transfers it, from its saliva into the bloodstream of its victim. The female anopheles mosquito is the usual vector and which injects the plasmodium parasite, the sporozoite, into the human blood stream. Here, they develop further until they are taken up during a blood meal by another mosquito which then looks for another victim to bite and inject with the sporozoites to continue to propagate the complex life-cycle. The most compelling thing about this stage of the disease is the formation of hypnozoites, a state that can endure for several weeks to even years before producing any obvious malaria attack.
There are five different species of the plasmodium parasite; there is the plasmodium falciparum and Plasmodium knowlesi which produce the most deadly infections. Then there are others, Plasmodium vivax, plasmodium ovale and plasmodium malariae which produce less serious infections and are thus considered to be less injurious than the former two species. However, the most common of these species is the P. falciparum. It is also the specie most commonly associated with the development of drug resistance. The P. falciparum is commonly found in the macaque monkeys native to South-East Asia but can also infect man with often severe consequences. This disease has infected man for thousands of years, right from the beginning of time. In ancient China, it was often the case that many sufferers were not cured unless they were given quinine or cinchona bark, or qiungaushu while the Caucasians were largely not in much contact with this disease. Those who did have contact with the disease died in large numbers and that represents one of the reasons why Africa was known as the dark continent or the Whiteman’s grave. During the 2nd World War, malaria accounted for significant morbidity and mortality among British troops as was the case among American troops during the Vietnam War.
Parasites injected into human blood stream destroy red blood cell and also invade the liver where they mature further before being released into the blood stream. That release coincides with the onset of a flu-like illness characterised by weakness, muscle aches, chills and nausea. This is soon followed by headache, fever, vomiting and sometimes diarrhoea. In more severe instances, there may be confusion, progressive loss of consciousness, convulsions and even coma. There may also be a dry cough and an inordinate urge to take drinks. Chills usually alternate with fever and sweating and this occurs every one, two or three days. The urine then becomes a deep yellow with associated bitter taste in the mouth which is almost invariably an indication that an individual has malaria. P. falciparum has an increased affinity for the proteins of well-nourished youngsters and pregnant women so that in these sub-populations, malaria is indeed a serious problem. It can cause abortions in early pregnancy and premature labour in more advanced pregnancies with the prospect of a high degree of foetal loss and of having low birth babies.
It sometimes goes beyond all these; it can cause severe bleeding disorders, shock, significant liver damage with jaundice appearing and kidney failure. The onset of coma is indicative of cerebral malaria, a situation in which the parasites get into the brain and interfere with certain important blood vessels. However, by far the most common complication seen especially in children and pregnant women is anaemia, a condition of inadequate blood count in a sufferer. In moderate and severe infections, the liver is consequently enlarged. The parasite can live in the liver in a dormant form for several weeks to even years before causing any disease. The incubation period of the infection varies from four to twenty-one days and so it is entirely possible to suffer from malaria twice a month. Certain types particularly P.vivax and P. ovale can live in that dormant form for up to eight months before causing any disease. It is thus possible for someone to recover fully from malaria and still harbour the parasites in the liver in enough numbers to start off a new infection soon afterwards.
Malaria is a problem in some 100 countries around the world mostly existing in a broad belt around the equator. It is also linked closely with poverty and it appears to be an accelerator of the HIV/AIDS pandemic as the two infections co-existing often tend to worsen the prognosis of the one another. It can be a difficult disease to diagnose. Clinically, it bears a strong resemblance to many other tropical diseases such as yellow fever, typhoid fever, dengue fever, cholera, filariasis and even measles. An African visitor to a Western country who comes down with malaria is likely to suffer a delay in diagnosis because of some of these similarities. Consequently, only a detailed travel history could point at the likely problem and it is thus considered a much better proposition to take preventive medications before leaving a malaria-endemic zone for one that is not. However, routine laboratory examination of the blood films of suspected sufferers should reveal the presence of the parasite. Sometimes, this is not definitive enough as it depends on the technical skill of the laboratory scientist who prepares the slides for giemsa staining and examination, and also on his ability to isolate the parasite once the slides have been prepared. More recent tests approved for use in the United States and elsewhere involve the utilisation of immunologic principles to determine the existence of the infection. There is the Rapid Diagnostic Tests which determine the presence of the plasmodium antigen in the blood sample of a suspected sufferer. The other one is the Polymerase Chain Reaction tests neither of which is commonly available in sub-Saharan Africa because of the relatively higher cost.
In spite of the overwhelming evidence of the degradation of the quality of life this disease causes in much of the Third World, there are many in Nigeria who derisively would say ‘I was suffering from ordinary malaria’. This is a warning that malaria is not ordinary. It causes a host of other problems than a loss of appetite, fever and vomiting and it is implicated in the deaths of at least 650,000 children under 5 years of age every year in Africa. It propagates poverty and contributes to poor school performance and attendance among sufferers, causes significant complications in all stages of pregnancy and is now seen to be an added burden for those who have HIV/AIDS and loss of valuable man-hours among workers.
ABUJA: Training Schedule for Basic Life Support BLS, Pediatric Advanced Life Support (PALS), Advanced Cardiovascular Life Support ACLS, First Aid, CPR, AED
PORTHARCOURT: Training Schedule for Basic Life Support BLS, Pediatric Advanced Life Support (PALS), Advanced Cardiovascular Life Support ACLS, First Aid, CPR, AED
LAGOS: Training Schedule for Basic Life Support BLS, Pediatric Advanced Life Support (PALS), Advanced Cardiovascular Life Support ACLS, First Aid, CPR, AED
STOP paying for airtime and electricity, Let your phone pay its bills with ScreenT
You may also like

PSN Raises Alarm as 3 Million Illegal Drug Outlets Threaten Public Safety
The Pharmaceutical Society of Nigeria, PSN, in Lagos State yesterday warned…

Agencies move to strengthen early warning systems in Nigeria’s healthcare sector
Key government and international agencies have intensified efforts to stren…
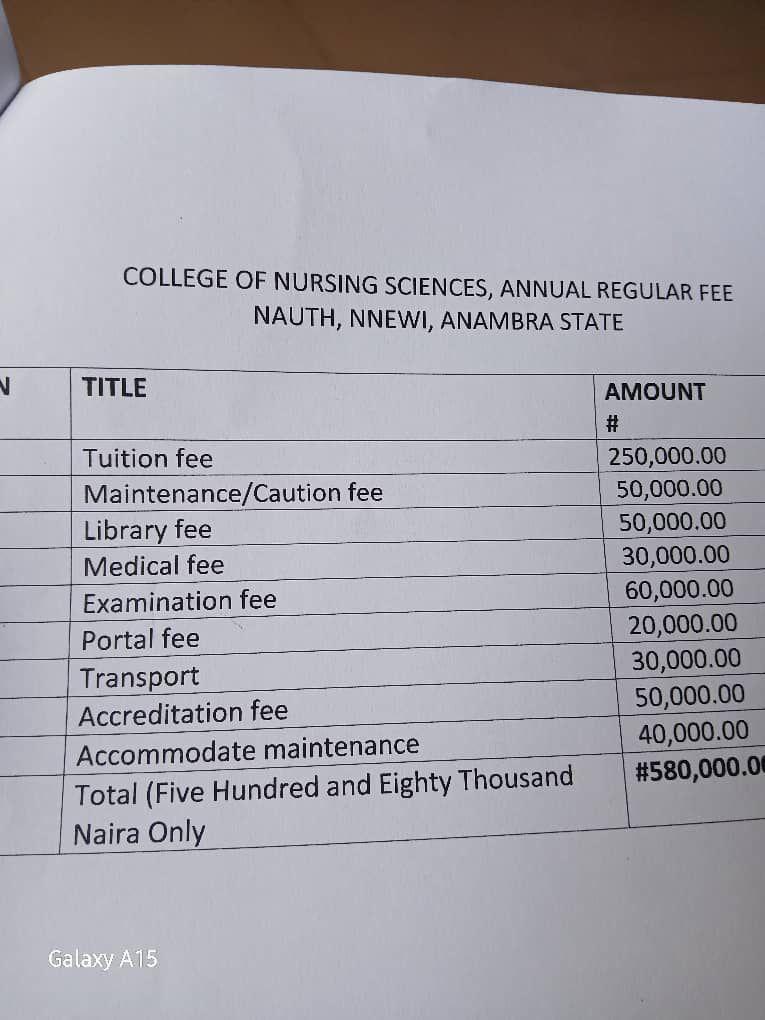
NAUTH management moves to resolve tuition hike protest, promises dialogue with students
The management of Nnamdi Azikiwe University Teaching Hospital (NAUTH) has p…

Child health outcomes improve as facility-based maternal deaths decline in 2025 FG report
The Federal Government has reported significant improvements in maternal, n…

World Kidney Day: Caregivers groan as dialysis hits N80,000 per session, transplant N30m
As the world marks World Kidney Day, caregivers and health experts in Niger…
